New thinking in management of ACL injury - Part II

The recent hubbub regarding the presence of the anterolateral ligament (ALL), and the re-examination of the anterolateral complex (AC) of the knee, stems from the conundrum of continued knee laxity - despite well constructed anterior cruciate ligament (ACL) repair. In the United States, surgeons perform between 75,000 and 100,000 ACL repairs are performed each year(1). Of those, instability remains in the knees of 11% to 30% of patients(1).
Graft failure usually gets the blame for residual knee instability after ACL repair surgery. However, even with technically well-executed repairs (when the graft should hold knee position), instability persists. Therefore, examiners have looked at the AC for secondary structures that aid in lateral knee stability. They concluded that the AC consists of extra-capsular fibres that in fact help stabilise the tibia at the knee joint.
Many refer to these fibres as the ALL; some contend they are deep fibres from the capsular-osseous layer of the illiotibial band (ITB), while others insist they are the mid-third capsular ligament. Studies report damage to the AC of the knee in up to 90% of knees thought to only have ACL injury(1). In fact, impairment in the AC correlates positively with an increase in severity of the pivot shift test(1).
A review by researchers at Virginia Tech/Carilion School of Medicine, found that when the AC is repaired with an extra-capsular tenodesis, (anchoring an existing tendon to better stabilise the joint), along with the intra-capsular ACL repair, pivot shift stability increases(1). In addition, when executed during an ACL repair revision surgery, the lateral tenodesis trended toward reducing revision failure. They also state that a lateral tenodesis may be appropriate for an athlete who tends toward joint laxity overall - a type of ‘belt and braces’ approach(1).
Surgeons at Barton Private Hospital in Australia performed revision ACL repairs on 38 adults(2). Eighteen of those still demonstrated a grade two or greater pivot shift immediately after revision. Those 18 patients then received an additional illiotibial band (ITB) tenodesis. The tenodesis procedure returned the pivot shift, anterior translation, and internal rotation of the tibia to normal.
A follow up two years later showed both groups - those with revision alone and those with the additional tenodesis - returned to similar levels of activity. If the tenodesis improves joint stability, why don’t all ACL surgical repairs include this augmentation? The reason is partly because the AC isn’t routinely evaluated in ACL tears. Also, a tenodesis that over corrects joint movement may increase the incidence of osteoarthritis (OA).
Why operate at all?
With the investigation into reasons for the high rate of failed or unsatisfactory ACL repairs comes the question, why repair the structure at all? Several assumptions lead to the promotion of a surgical option:- The ACL is unable to heal due to lack of blood clot formation.
- The alteration of joint motion in an ACL deficient knee leads to meniscal injury;.
- An unrepaired ACL tear increases the chance for joint degeneration and early onset OA.
- A knee without an ACL impairs function and prevents return to sport.
However, scholars are starting to challenge some of these assertions and take another long look at conservative treatment as an option for ACL injury. Researchers at Erasmus University in Rotterdam recently released the findings of a 20-year follow-up study of 50 high level athletes with ACL injury(3).
After initial injury, all athletes received three months of rehabilitation. Investigators offered the opportunity to receive surgical repair to athletes who did not respond positively to conservative management within this time frame. Ten years after initial intervention, they divided patients into two groups (those who had received operative and those who had non-operative management). These patients were pair matched (according to age, gender, and performance level prior to injury), evaluated; and then followed for another twenty years (see table 1).
During the 20-year follow up, the number of meniscectomies (four knees in the operative group and 10 knees in the conservative group) was not significant. Thus not repairing the ACL did not place the athletes at greater risk of meniscal injury. The incidence of joint deterioration in the injured knees was 80% in the operative group and 60% in the conservative group. While differing somewhat, these numbers also did not reach a level of significance.
After the initial injury, both groups experienced a slight decrease in activity level, from Tegner scores of 9 prior to injury, to eight in the operative group and seven in the conservative group. At ten years after injury, the operative group’s median Tegner score was six and the conservative group’s was five. Twenty years later, the scores were five and four, respectively. Even after 20 years, measures of physical activity did not differ significantly between the groups. In addition, the change in function between the 10-year and 20-year follow up was not significantly different within either group. There are some potential criticisms of this study (see box 1) but given the results, it seems reasonable to conclude that both conservative and operative treatments may be equally effective, and that it could be logical to try a conservative approach first.
| While this study points to the fact that conservatively managed knees do just as well as surgically repaired knees, bias in the initial population selection should be noted. Athletes were not randomly assigned to groups. Rather, those that responded well to three months of initial therapy continued conservative management. Those with symptomatic and persistent instability after three months were offered surgical repair.The study also lacks details of the initial conservative protocol, except to refer to a minimum three-month period of intense hamstring and quadriceps strengthening. Furthermore, the patients with subjective complaints of residual instability and giving-way after three months were given the choice of surgical repair or a change in lifestyle (to avoid cutting/pivoting activities). There is therefore a possibility of suggestive bias in those patients — ie were they convinced from the start that surgery was the only option to return to the lifestyle that they enjoyed?The patients were initially diagnosed on MRI or arthroscopically, with no mention of the AC. The authors didn’t give any results of clinical examinations after injury either. It would be interesting to know which of the knees also suffered damage to the AC. Without graded clinical exams, (which have been shown to correlate with AC deficit), it’s impossible to say why some responded well to initial treatment and others did not. Did the knees with persistent instability also suffer more significant damage to the secondary stabilisers in the AC? Questions therefore remain in regard to decision making, and forming an algorithm from which to choose the right approach. |
| Operative Treatment | Conservative Treatment | P - Value | ||
|---|---|---|---|---|
| n = 25 | n = 25 | |||
| Gender (men/women) | 19/6 | 19/6 | 1.000 | |
| Age (years), mean (+/- SD) | 37.6 (6.2) | 37.8 (6.8) | 0.808 | |
| BMI, median (min-max) | 25.3 (22.2-30.9) | 24.9(20.9 - 28.7) | 0.443 | |
| Preinjury Tegner score, median (min-max) | 9 (6.0-10.0) | 9 (6.0 - 10.0) | 0.831 |
Investigators matched subjects in each group based on age, gender and Tegner score. The Tegner scale is a measure of participation in activity - from zero (sick or disabled due to knee injury) to 10 (competitive sports such as football, rugby).
Guidelines for conservative management
While isolated unilateral ACL tears likely present the best prospects for positive outcomes from conservative management, researchers at the University of Pittsburgh suggested additional criteria for decision making(4). Using these measures, 79% of athletes selected for conservative treatment returned to their sport and completed their competition season without further incidence of their knee ‘giving way’(4). They include:- A six meter timed hopping test score on the injured leg equal or greater than 80% of the score of the uninjured leg.
- A score of 80% or better on the ‘Knee Outcome Survey of Activities of Daily Living’.
- A ‘Global Rating Scale’ of perceived function score of 60% or more six months after injury.
- Only one episode of knee instability between injury and evaluation.
The goal of rehabilitation is to return the athlete to full sports participation. Without the donor site or graft integrity to consider, progress moves more swiftly through the early stages of recovery. During the acute period, a typical course of impairment-based rehab addresses swelling, strength, endurance, weight bearing as tolerated, and range of motion, alongside activity modification and bracing as needed.
Once stable, neuromuscular training enhances ability to return to sport. The ACL contains mechanoreceptors and free nerve endings, which are thought to contribute to the stability and position sense of the knee. Without this input, neuromuscular compensatory patterns must be trained in order to return to pivot and cutting activities. To accomplish this, consider stimulating to all levels of the nervous system when planning therapeutic activities (see figures 1a and b).
For instance, double and single-leg stance on uneven surfaces, and plyometrics challenges neuromuscular control at the spinal cord level. Manipulating both the base of support and visual input elicits brain-stem balance reactions. Foster the athlete’s conscious awareness of body position using external feedback, and verbal cues such as, “Jump and land with your knees bent to 45 degrees.” Progress the athlete rapidly towards relying on internal feedback using instructions that incorporate function, such as, “Jump and land in a squat.” This allows the athlete to focus on how the body feels in space and what control is necessary to achieve the goal, rather than a specific movement (see figure 2). Finally, place the athlete in functional situations and remove all verbal cues.
Figure 1a: Proprioceptive neuromuscular training

To return to sport, athletes need proprioceptive neuromuscular training, especially without an ACL. Manipulate variables of base of support, visual input, and single or double limb stance, progressing difficulty and incorporating sports specific tasks as tolerated.
Figure 1b: High level proprioceptive training
Australian physiotherapist and ACL guru Mick Hughes promotes high -evel proprioceptive training, which simulates performance situations. When ready to return to sport-specific training, continue with partner push drills to increase readiness for performance. The athlete jumps and is pushed from any direction. The key to the drill is landing with good form, first on both feet and then on just one. (Photos used with permission(5))

Figure 2: Using internal feedback
In a narrative review, researchers in the Netherlands found that when instructed to keep the knee over the toes in a split squat (photo a), the athlete relies on external verbal cues to perform the activity. He focuses on following the instructions for the knee, and loses control at the hip. When instructed to perform the targeted task of moving his knee toward the cone (photo b), the athlete feels and controls body movement, as noted in the decrease in hip adduction(6). (Photos used with permission.)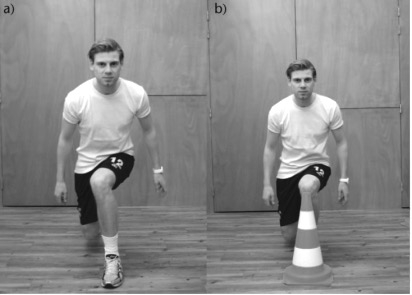
Case study: Professional footballer
Despite the fact that two surgeons recommended surgical repair, a 32-year old male professional footballer in the English Premier League took a chance on conservative management of his non-contact ACL tear in order to attempt to finish out the competitive season(7). MRI revealed a complete ACL tear with bone bruising, oedema, and grade-I injury to the medial collateral ligament of his right knee. The athlete and consulting medical team agreed to an initial week of rest and modalities to decrease swelling, followed by four weeks of rehabilitation and monitoring.Since diagnostic tests are no measure of perceived instability, and unchanging if the ACL remains torn, the patient performed single leg hop and crossover tests every two to three days to evaluate progress (see figure 3). He indicated level of trust in his knee stability daily, using a modified Likert scale. The rehab protocol included ample recovery, allowing only two to three consecutive days of exercise before taking a rest day.
The rehabilitation began in the gym with an athlete-centred approach. The rehab team considered which activities the athlete preferred when planning treatment. They hypothesised that this interactive approach may have improved outcomes by allowing the athlete to better cope with his injury by ‘feeling in control’. The initial program focused on strengthening the legs, specifically the quadriceps, using high-volume reps and sets with low resistance. Exercise progression increased weight while simultaneously decreasing volume.
The athlete tolerated exercise well, showing no adverse effects such as increased swelling or pain. Therefore, the program advanced to low-level plyometrics and single-leg proprioceptive training. Therapists employed electrical stimulation, occlusion training, and time under tension throughout the rehabilitation, to promote muscle recruitment and strength gains.
After the seventh rehab session, the athlete began running training at 70% of body weight using an antigravity running machine. Once he had increased to 90% of body weight, he started outside running sessions, beginning at below 50% of his maximum speed. The athlete progressed through sport-specific cutting, turning, and jumping drills to high-intensity running. By seven and a half weeks post injury, the athlete moved from developmental squad training sessions to practicing with the first team. He went on to play in five first-team matches before the season ended. At the time of publication of this study, eighteen months after injury, the athlete played as a starter for the first team. The authors site the patient’s participation in the process through open communication, fully informed consent, and joint decision making, to contribute significantly to the positive outcome.
Figure 3: Hop tests

Time the athlete as he/she hops for six meters (right hand graphic). Take the average of two timed trials. Record the difference as a measure of impairment and potential for conservative management. Record subsequent times to indicate response to therapy.
Conclusion
The ACL is the most frequently torn ligament in the knee. Typically, these injuries are treated with surgical repair. However, knee instability often remains, despite well executed surgical intervention. The structures in the AC of the knee appear to act as secondary stabilisers. Therefore, residual instability may be caused by insufficient healing in the AC which could be improved with a lateral tenodesis procedure.Research shows that even if the knee remains unstable, with or without an ACL repair, appropriate rehabilitation enables high-level athletes to return to sport without an increased risk of meniscal damage or osteoarthritis. If returning to play due to timing and sport season commitments is important to the athlete, conservative management is a viable, faster, and safe option. Fully explain the risks and benefits of each approach, monitor constantly, and involve the athlete intimately in the rehab planning process for the best chance at success.
References
- Clin Sports Med. 2018;37:101-13
- Am J Sports Med. 2018 Jan;Epub ahead of print
- Am J Sports Med. 2018 Feb;Epub ahead of print
- 2000;30(4):194-203
- Twitter @mickhughes
- EFFORT Open Rev. 2017 Oct;2:410-20
- BMJ Case Rep. 2015 April 26;Epub
You need to be logged in to continue reading.
Please register for limited access or take a 30-day risk-free trial of Sports Injury Bulletin to experience the full benefits of a subscription. TAKE A RISK-FREE TRIAL
TAKE A RISK-FREE TRIAL

Alicia Filley

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up
Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.