Ankle deep in the wrong diagnosis
Any number of pathologies produces lateral heel pain. As Chris Mallac explains in the first instalment of his master class on chronic ankle instability (CAI), lateral heel pain is often the result of repeated ankle sprain. Mallac goes on to describe how CAI can lead to sinus tarsi syndrome, causing lateral heel pain and rear foot instability. Alicia Filley further explains how some theorize that chronic ankle instability arises from undiagnosed peroneal dysfunction.

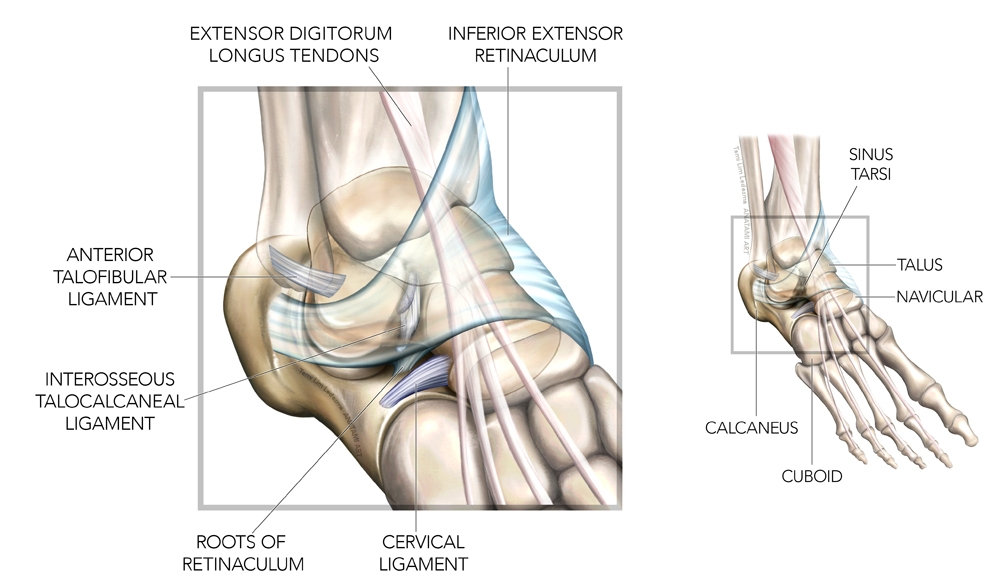
Any number of pathologies produces lateral heel pain (see table 1). As Chris Mallac explains in the first installment of his master class on chronic ankle instability(CAI), lateral heel pain is often the result of repeated ankle sprain. Mallac goes on to describe how CAI can lead to sinus tarsi syndrome, causing lateral heel pain and rear foot instability (see figure 1). Alicia Filley further explains how some theorize that chronic ankle instability arises from undiagnosed peroneal dysfunction after an inversion injury. That dysfunction can occur in the form of tendinopathy, subluxation or dislocation, and splits or tears, all of which can produce lateral heel pain.
| Peroneal dysfunction: tendinopathy, splits/tears, or subluxation/dislocation |
| Inversion injury |
| Sinus tarsi syndrome |
| Calcaneal stress fracture |
| Distal fibular fracture (Salter-Harris in pediatrics) |
| Calcaneal apophysitis |
| Sural nerve injury / neuropathy |
Figure 1: Sinus tarsi anatomy
What about lateral heel pain that occurs without an inversion injury? It’s possible that the injury was so slight and inconsequential that the athlete may not remember it, yet it was enough to strain the peroneal muscles. Pain from peroneal strain can arise a day or so after the incident. If the load on the peroneals remains high, tendinopathy can develop.
Such was the presumed diagnosis of a 16-year-old male cross-country runner who presented to the clinic with a one-week history of right-sided lateral heel pain when running. His pain was vague, generally in the area under the lateral malleolus, and difficult to reproduce in the clinic with passive or active mobility, resistance, orthopedic tests, or running on a treadmill. He reported the pain improved with rest and then came back after running more than a mile with his track team. Afraid of hurting himself further, he stopped running as soon as he felt the discomfort.
The athlete was prescribed relative rest, modification of running program to run one to three minute intervals at a recovery pace on the treadmill within pain tolerance, and peroneal muscle resistance exercises. The patient returned two weeks later with no improvement of symptoms. In fact, he could no longer tolerate running short intervals and had stopped running altogether. He cross-trained on the stationary bike, which did not exacerbate his symptoms.
It took an outdoor run and plyometric workout with the physio to aggravate the problem enough for the athlete to pinpoint the location of his pain. When pushed beyond his initial discomfort threshold, the actual site of pain was further down the heel along the lateral border of the calcaneus. The athlete suffered not from peroneal tendinopathy, but from calcaneal apophysitis, also known as Sever’s disease.
Sever’s disease is an overuse injury common in adolescents. The injury occurs at the calcanea apophysis, which is both the site of the calcanea growth plate and the insertion of the Achilles tendon (see figure 2). It happens primarily in adolescents who experience rapid and sudden growth spurts, participate in year-round sports, experience a sudden increase in training load, or perform sports that require running and jumping. Achilles tightness, worn out shoes, hard surfaces, and a weak anterior tibialis may contribute to the problem. Other causative factors may include genu varum, high medial arch and forefoot varus, and over-pronation.
Figure 2: Achilles tendon attachment
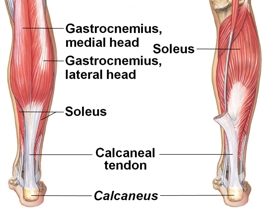
Illustration of Achilles tendon, here called the calcaneal tendon, into the calcaneus.
Calcaneal apophysitis most often strikes adolescents between the ages of nine and 12. Symptoms are bilateral in 60% of cases(1). It occurs in boys more than girls. The mechanism of injury is micro trauma to the apophysis from the tension created as the leg bones grow more rapidly than the muscles. With continued sports participation, the vulnerable area becomes irritated and painful.
Physical exam reveals no evidence of trauma. The area of insertion may be painful to palpation, dorsiflexion stretch, or standing on tiptoes. The calcaneal squeeze test is diagnostic if positive (see figure 3). Treatment is symptomatic, aimed at decreasing pain and making the athlete more comfortable. It usually consists of rest, cross training, and load management to allow the athlete to train but remain below their pain threshold. The use of heel cups or lifts decreases tension on the tendon. Use complete immobilization if the pain is severe. Gentle Achilles stretching can stimulate lengthening the muscle but refrain from placing more tension on the calcaneus.
Figure 3: The calcaneal squeeze test

If pressure on either side of the Achilles at the attachment to the calcaneus elicits pain then the test is positive for Sever’s disease.
Sever’s disease usually resolves on its own, but may take six to 12 months. As the muscles lengthen the tension on the apophysis lessens. Injection therapy and surgical intervention is not recommended, despite the possible long recovery. Frustrated athletes may have to sit out a season. As in the case of the cross-country runner, time revealed all. He grew nearly two inches in the next six months. He missed not only his cross-country season but track as well. However, he continued to run within his pain tolerance on alternating days, used stationary bike workouts to build his endurance, and continued with his strengthening program. He also employed the use of heel cups for symptomatic relief. Although athletes may struggle with the down time out of sport, keeping up strength and endurance means they will come back ready for competition with healthier and bigger bodies.
Reference
- StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019-May 6
You need to be logged in to continue reading.
Please register for limited access or take a 30-day risk-free trial of Sports Injury Bulletin to experience the full benefits of a subscription. TAKE A RISK-FREE TRIAL
TAKE A RISK-FREE TRIAL

Alicia Filley

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up



Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.