Roll away the blues

The use of foam rollers to provide tissue massage has become very popular in recent years. Advocates for foam rolling cite a number of potential benefits for its use. These include improved joint mobility and flexibility, enhanced recovery following intensive exercise where delayed onset muscle soreness (DOMS), a reduction in fascial tissue stiffness and a reduction in injury-related pain. There’s even some suggestion that regular foam rolling could enhance muscle force generation and by doing so, improve athletic performance. In this article, we will look at the most recent evidence to support (or otherwise) these claims, and the most effective implementation protocols for foam rolling.
Foam rollers come in several sizes and densities. Commercial foam rollers are typically available in two lengths: 36 inches and 18 inches(1). The structure of foam rollers vary from a mild density foam to a more rigid and solid plastic cylinder with a dense foam outer covering.
Although researchers have demonstrated that higher density foam rollers can produce more pressure on the target tissues than softer density foam rollers(2), the downside is that some patients may find hard foam rollers too uncomfortable to use so a compromise may be needed. The foam rolling surface may also vary from smooth to textured, through to ‘knobbly’. To date, there’s little evidence in the literature as to which surface type may be most effective; however, the ‘GRID’ foam roller (see figure 1) has been used in previous studies in this area with positive results(3,4).
Figure 1: A ‘GRID’ foam roller

Questions
The practice of foam rolling has only really become popular in the last decade or so. And while studies have reported various beneficial results from a foam-rolling programme, there remain a number of questions to be resolved. Examples of these questions include:- How effective is foam rolling for increasing joint range of movement (ROM)?
- Can foam rolling techniques be effectively self taught?
- Which types of rollers are most efficient?
- Is foam rolling an effective technique for myofascial tissue release?
Unfortunately, the relatively limited amount of evidence available to date means that it’s not possible to fully answer all of these questions; however a look at some of the more recent studies can give clinicians some useful insight into what are likely to be effective approaches.
Foam rolling and ROM
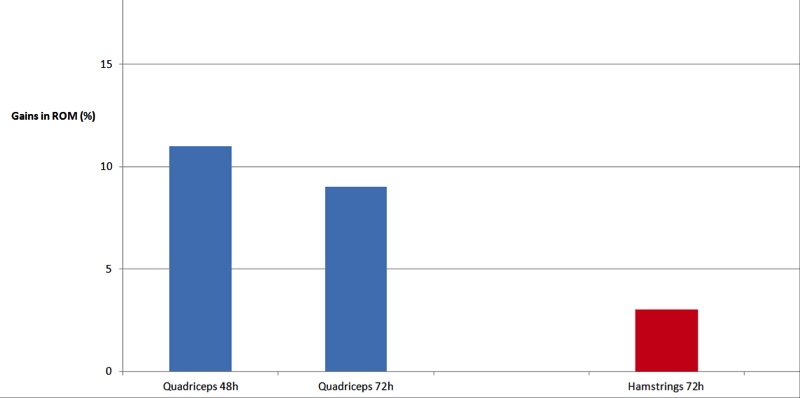
Many studies have investigated how stretching affects range of motion and performance. In general, these results showed increased ROM following a stretching programme but with (in the short term) an impairment in subsequent performance – an undesirable outcome for an athlete who is seeking to improve joint flexibility in readiness for competition or training(5,6).More recently, the use of foam rolling has been advocated as an alternative to stretching. In a study that have examined how a foam roller affects flexibility, researchers reported 12.7% and 10.3% increases in knee-joint ROM at two minutes and ten minutes respectively, following two 1-minute bouts of foam rolling(7). In another study, researchers found that compared with no foam rolling, quadriceps ROM was 11% and 9% greater at 48 hours and 72 hours, respectively after treating exercise-induced muscle damage (EIMD) with a foam roller (see figure 2)(8). In the same study, hamstring flexibility at 72 hours post foam rolling was 3% greater.
Figure 2: Improvements in range of movement following foam rolling(8)
In a study in which roller massagers (hand-held rollers applied to the muscles with force applied by the user rather than using bodyweight – see figure 3), researchers demonstrated a 4.3% increase in ‘sit-and-reach’ ROM with 5 and 10 seconds of roller-massager application(9). Although not significant, they found a trend for 10 seconds of roller massaging to increase ROM more than 5 seconds. Importantly – and contrary to most static-stretching studies involving prolonged durations – all three of these studies reported either no subsequent reduction in voluntary force or activation, or a much lesser degree of impairment.
Figure 3: Roller massager

Another study looked at the effects of roller massaging on knee ROM and neuromuscular efficiency during the lunge exercise(10). Ten recreationally active participants performed three randomised experimental trials on three separate occasions:
- Five repetitions of 20 seconds of roller massaging to the quadriceps.
- Five repetitions of 60 seconds.
- A control condition in which participants sat quietly.
To ensure consistency, the rolling was applied by a machine set at 25% of each participant’s body mass. The two key findings were as follows:
- Knee-joint ROM was 10% and 16% greater than the control condition in the 20-second and 60-second roller-massager conditions, respectively.
- A roller massager applied to the quadriceps at a load equal to 25% of body mass was moderately painful and induced minor contractions as measured by (EMG).
More evidence
Further studies also provide credibility to the notion that both foam rolling and roller massaging can aid in improving range of motion. For example, in a study on 40 subjects with less than 90 degrees of passive hip-flexion ROM, researchers compared the effects of foam rolling and static stretching on range of motion(11). During each of trial sessions, subjects' passive hip-flexion ROM was measured before and immediately after the following:- Static stretching only
- Static stretching combined with foam rolling
- Foam rolling only
- Nothing (control)
To minimise accessory movement of the hip and contralateral leg, the subjects adopted a supine position, with a strap placed across their hip, and another strap located over the uninvolved leg just superior to the patella. A bubble inclinometer was then aligned on the thigh of the involved leg, with which subjects then performed hip flexion. The results showed that that both static stretching and foam rolling produced gains in passive hip-flexion ROM. Interestingly, a combination of the two produced slighter greater ROM gains, which led the researchers to conclude:
‘Our results support the use of a foam roller in combination with a static-stretching protocol. If time allows and maximal gains in hip-flexion ROM are desired, foam rolling the hamstrings muscle group before static stretching would be appropriate' (11).
Another study compared the effects of static stretches and self-administered roller massaging of the calf muscles on ankle ROM, maximal voluntary contraction (MVC), force F100 (force produced in the first 100ms of the MVC), electromyography (EMG of soleus and tibialis anterior) the characteristics of the plantar flexors, and a single limb balance test in 14 recreationally trained subjects(12).
After a warm up, subjects were assessed for passive dorsiflexion ROM, MVC, and a single-limb balance test with eyes closed. Following the pre-test, participants randomly performed either static stretches or roller massaging (three 3 sets of 30 seconds, with ten seconds of rest between each set). Both roller massage and static stretching increased ROM immediately and 10 min after the interventions. However, when maximum voluntary contraction was also assessed after 10 minutes, the self-massage with a roller massager led to significant improvements in MVC force compared to stretching.
Foam rolling for myofascial release
Self-myofascial release (SMR) is an intensive self-treatment with rigid foam rollers and other small handheld tools based on the exertion of compressive force to the soft tissue. Often these tools are used as part of a comprehensive program and are often recommended to the client to purchase and use at home Aiming to tackle dysfunctions of the skeletal muscle and connective tissue, it claims to mimic the effects of manual therapy techniques. As we’ve seen, recent studies indicate that SMR, among other things, improves range of motion without concurrent decrease in neuromuscular performance.In addition to neuronal mechanisms, such as increased stretch tolerance(13,14), these flexibility increases might be attributed to acute two key morphological adaptations:
- The fasciae surrounding the muscles of the lower extremity are composed of multiple fibrous layers. Loose connective tissue enriched with hyaluronic acid allows these layers to slide against each other during motion – for example contraction or elongation of the underlying muscle – see figure 4)(15). Several researchers have postulated a positive effect of SMR using foam rolling on fascial sliding properties. This effect may come about by breaking up adhesions or loosening cross-links between these layers(1,16).
- Another hypothesised morphological consequence of SMR is the alteration of passive tissue stiffness, such as that which occurs after static stretching. A number of studies have demonstrated the existence of myofibroblasts (and their ability to impact stiffness) in fascia(17,18). According to in vitro experiments, fascial hydration has been shown to alter biomechanical tissue properties(19). Therefore, compression of the muscle and the surrounding fascial tissue by use of a foam roller might stimulate contractile cell activity, and beneficially affect tissue hydration and the microarchitecture of cell cytoskeleton or muscle filament mechanical properties - and thereby reducing fascial tissue stiffness(20,21).
But while both of these morphological mechanisms seem highly plausible, there is insufficient scientific evidence to date to confirm that this is the case. That’s because most studies have focussed purely on functional and subjective parameters such as flexibility, range of movement, recovery and pain. However, there is currently a trial underway to try and explore the underlying mechanisms involved in self-fascial release using a foam roller or roller massager(22). In this study, researchers are evaluating the acute effects of SMR on the passive tissue stiffness of the anterior thigh muscles, and the sliding properties of the associated fasciae. Results are expected in the near future.
Figure 4: Fasical architecture
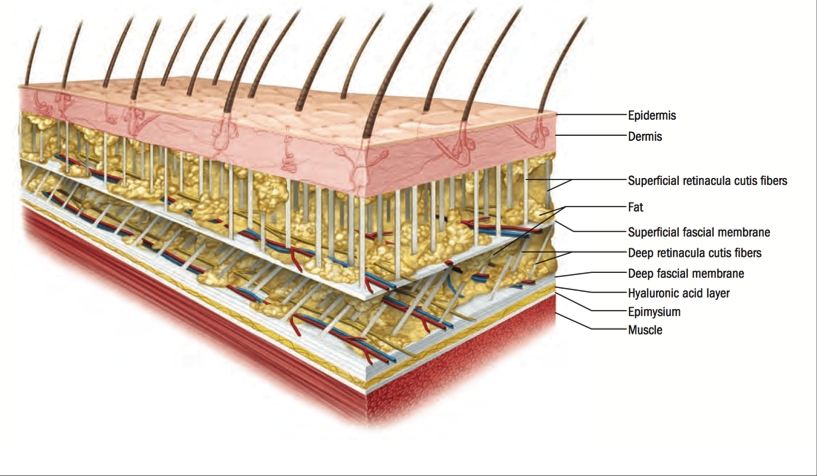
Cross section from skin to the musculature, showing fascial membranes and hyaluronic acid layer
Which foam roller?
Readers will have noticed that both foam rollers and roller massagers have been shown to produce beneficial effects in studies. This begs the question as to which type might be more effective. A study published earlier this year compared the effects on flexibility of foam rolling vs. roller massaging of the hamstrings(23). In particular, the researchers sought to establish whether foam rollers and roller massagers were equally effective for increasing hamstrings flexibility in asymptomatic physically active adults. Looking at data from previous studies on foam rolling and roller massaging, four studies were analysed – two using roller massagers and two using foam rollers.Both of the roller-massager studies reported significant increases in hamstrings flexibility after treatment. Meanwhile, the data from the foam-roller studies did not seem to demonstrate a statistically significant increase in hamstring flexibility, although one of the two studies did demonstrate a strong effect that nearly reached significance. The authors concluded that moderate-quality studies support the use of roller massagers but provide limited evidence on the effectiveness of foam rolling to increase hamstring flexibility. They suggested that the superior result observe in the roller massaging studies was likely due to a longer a longer duration of treatment and administration by a trained therapist rather than any mechanical effect of the rollers themselves.
The results from the study above seem to hint that for the best outcome, the application of a roller (foam or massager) is best carried out by a trained therapist. However, a study also published earlier this year suggests that this is not necessarily the case. In this study, researchers set out to compare the effects of video-guided, live instructed, and self-guided foam rolling interventions on knee flexion ROM and pressure pain thresholds in 45 adults(3). Subjects were recruited and randomly allocated to one of three intervention groups (see box:
- Video-guided
- Live-instructed
- Self-guided
Each foam rolling intervention lasted a total of two minutes and the variables measured included knee flexion ROM and pressure pain threshold of the left quadriceps.
The results showed that all three of the intervention groups showed significant gains in knee flexion ROM and pressure pain thresholds (an approximate 5-degree increase of knee flexion and a 150kPa increase in pressure pain threshold). Moreover, all the tuition methods showed the same magnitude of gains, and the researchers concluded that clinicians can confidently use video or self guided techniques to help their clients perform foam rolling interventions independently outside of formal care.
Methods of instruction(3)
- For the video-guided intervention, subjects followed an instructional video that demonstrated the use of the foam roll on the left quadriceps muscle group. Subjects had their own foam roll and followed the investigator. The instructor in the video provided a brief introduction and then discussed the foam rolling technique.
- For the live-instruction intervention, subjects followed the examiner’s instructions, which were the same as the video-guided intervention. The video was transcribed into a text-based script that the examiner followed while teaching the foam rolling technique. The examiner began by demonstrating the foam-rolling sequence then had the subject perform the two-minute sequence of rolling and knee bends.
- For the self-guided or control intervention, the primary investigator demonstrated the plank position and placement of the roller under the left quadriceps group. Subjects performed their own preferred method of foam rolling on the left leg for two minutes. The investigator monitored the intervention time and did not provide any feedback.
Vibrating rollers
Finally, it’s worth mentioning a new type of foam roller, which has recently appeared on the market. Recently, manufacturers have combined technology of vibration therapy with foam rolling – and come up with the development of vibrating foam rollers. But are they more effective? Until just a couple of months ago, there were no peer-reviewed investigations on this technology. However, a study recently published looked at the effects of a vibrating roller and non-vibrating roller intervention on prone knee flexion passive range of motion (ROM) and pressure pain thresholds (PPT) of the quadriceps musculature(24).Forty-five recreationally active adults were randomly allocated to one of three groups:
- Vibrating roller
- Non-vibrating roller
- Control
Each rolling intervention lasted a total of two minutes while the control group did not roll. Measured outcomes included prone knee flexion ROM and PPT. The vibrating roller demonstrated the greatest increase in PPT (180kPa), followed by the non-vibrating roller (112kPa), and control (61kPa). For knee ROM, the vibrating roller demonstrated the greatest increase in ROM (7 degrees), followed by the non-vibrating roller (5 degrees), and control (2 degrees). In terms of significance, the gains in ROM vibrating and non-vibrating rollers were of similar magnitude (although there was a trend towards great ROM with the vibrating roller). However, the results clearly showed that a vibrating roller may increase an individual's tolerance to pain greater than a non-vibrating roller. With such a paucity of research, it’s too early to be 100% confident that a vibrating roller could be superior to a non-vibrating roller, but the initial results are certainly encouraging.
Summary
Recent studies seem to confirm that foam rolling and roller massaging are capable of improving joint ROM across a number of joints. The effects are equivalent or superior to static stretching but without the acute performance drawbacks of the latter. Foam rolling may also be effective for self-myofascial release, although the mechanisms by which these benefits are realised remain to be elucidated. Foam rolling can be successfully used by clients outside of the clinic setting providing instruction is given – either verbal, video or self-guided. Vibrating rollers may give additional benefits in terms of pain tolerance but more research is needed to confirm this.References
- J Bodyw Mov Ther. 2015;19(4):747-758
- J Sport Rehabil. 2008;17(4):432-442
- Int J Sports Phys Ther 2017; (12)2 242-249
- IntJ Sports Phys Ther. 2015;10(2):203-212
- Eur J Appl Physiol. 2011; 111(11):2633–2651
- Med Sci Sports Exerc. 2012;44(1):154–164
- J Strength Cond Res. 2013;27(3):812–821
- Med Sci Sports Exerc. 2014;46(1):131–142
- Int J Sports Phys Ther. 2013;8(3):228–236
- J Athl Train 2015;50(2):133–140
- J Sport Rehabil. 2014 Nov;23(4):296-9
- Int J Sports Phys Ther. 2014 Feb;9(1):92-102
- J Athl Train. 2015;50:133–40
- J Strength Cond Res. 2015. doi:10.1519/JSC.0000000000001007
- J Bodyw Mov Ther. 2008;12:225–30
- J Bodyw Mov Ther. 2013;17:103–15
- Manuelle Medizin. 1996;34:196–200
- Med Hypotheses. 2005;65:273–7
- J Bodyw Mov Ther. 2012;16:94–100
- Nature. 2010;463:485–92
- Nature. 2007;445:295–8
- Trials201718:114 doi.org/10.1186/s13063-017-1866-y
- J Sport Rehabil. 2017 Jan;26(1):94-100
- J Sport Rehabil. 2017 Aug 8:1-23
You need to be logged in to continue reading.
Please register for limited access or take a 30-day risk-free trial of Sports Injury Bulletin to experience the full benefits of a subscription. TAKE A RISK-FREE TRIAL
TAKE A RISK-FREE TRIAL

Andrew Hamilton

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up




Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.