You are viewing 1 of your 1 free articles
Practice makes progress: evidence, experience, and expectations in rehabilitation design

INTRODUCTION
An evidence-based approach is “the conscientious, explicit, and judicious use of the current best evidence in making decisions about the care of individual patients”(1). It represents the aim of Sports and Exercise Medicine (SEM) practice. The hierarchy of scientific evidence for health research ranks different types of evidence. It suggests that where possible, we should use interventions that demonstrate effectiveness in meta-analysis or systematic reviews, or at the very least, a randomized controlled trial (see figure 1).Figure 1: The hierarchy of evidence for health research
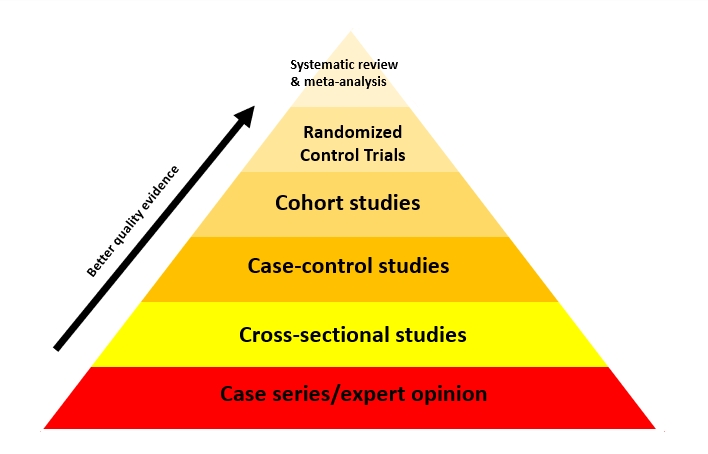
However, evidence-based practice has its roots in medicine, and medical research is commonly binary. For example, researchers typically design studies to establish the efficacy of a particular treatment compared to a control group (no intervention) or to compare different treatment options.
THE SCIENCE-PRACTICE GAP
Injury rehabilitation is different from clinical medicine, and professionals working in these spaces generally aren’t presented with binary choices. Practitioners have the option to choose between and combine multiple therapies—for example, acute injury management with ice, elevation, and immobilization or early mobilization and loading. Adjunctive therapies offer other treatment options, for example, manual therapy, ultrasound, laser, dry needling, cupping, shockwave therapies, and exercise prescription. Exercise prescription alone presents many adjustable parameters (frequency, volume, velocity, and intensity) that will influence treatment outcomes. While each aspect of treatment may have supporting scientific evidence, it is rare for research to investigate the interactions of different therapies that could reasonably complement each other. The ‘science-practice gap’ is the disparity between research results and their applicability in clinical practice. A six-step plan may address the development of evidence-informed rehabilitation, which narrows the gap between the evidence base and clinical practice.EVIDENCE-BASED PRACTICE
To narrow the ‘science-practice gap,’ medical researchers advocate for evidence-based practice that increases scientific research awareness, interpretation, and implementation by healthcare professionals. However, practitioners need to apply the knowledge appropriately in their clinical context using clinical experience and understanding athlete preferences (see figure 2). For example, blood flow restriction (BFR) therapy could help maintain muscle mass and strength in an athlete with a long-term lower limb injury. However, clinical experience identifies that although BRF allows for muscular metabolic stress at lower loads, it is often difficult for athletes to tolerate. As a result, practitioners may need to use alternative treatment modalities despite the evidence base to support BFR. Thus, evidence-based practice is not the selection of treatment modalities supported by evidence but rather appropriate clinical reasoning to identify the athlete’s most appropriate holistic treatment modality.Figure 2: Evidence-based practice
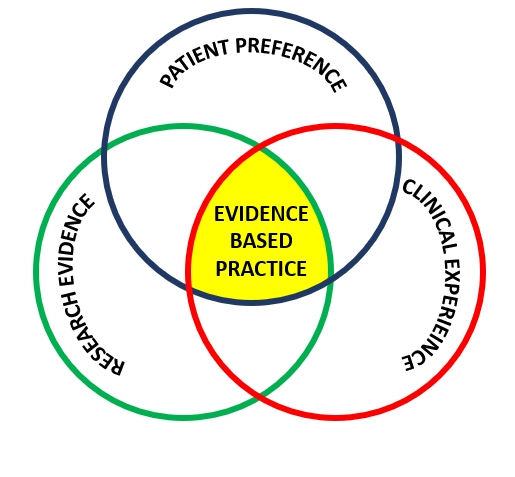
Evidence-based practice acknowledges that decisions regarding treatment plans will be based on clinical experience, informed by research evidence, and determined by patient preferences. However, practitioners may make errors in judgments due to unpredictable responses and natural biases. Therefore, it is important to design systems that mitigate errors in judgment.
PRECISION MEDICINE: AN INDIVIDUALISED APPROACH
The health sciences industry widely accepts that the responses to medical treatment and therapies may vary amongst individuals. Therefore, the treatment response will influence clinical decision-making. Athletes can be classified into three broad groups when assessing their response to treatment: adverse responder, non-responder, or extreme responder. Practitioners need to understand that treatment plans are judgment calls and thus are subject to human error. For example, a graded and criteria-based rehabilitation plan is necessary to optimize anterior cruciate ligament reconstruction rehabilitation. However, the introduction of inappropriately timed loads may lead to re-injury.The precision medicine approach advocates using biomarkers such as DNA, hormones, or blood markers to evaluate the response to treatment. In the case of injury rehabilitation therapies, few biomarkers exist that inform the likely response to treatment, but it is possible to measure key variables to determine rehabilitation progress. Frequent objective and subjective re-assessment will provide practitioners with valuable information to evaluate progress and guide the manipulation of rehabilitation parameters and protocols.
EVIDENCE-INFORMED SIX-STEP PLAN
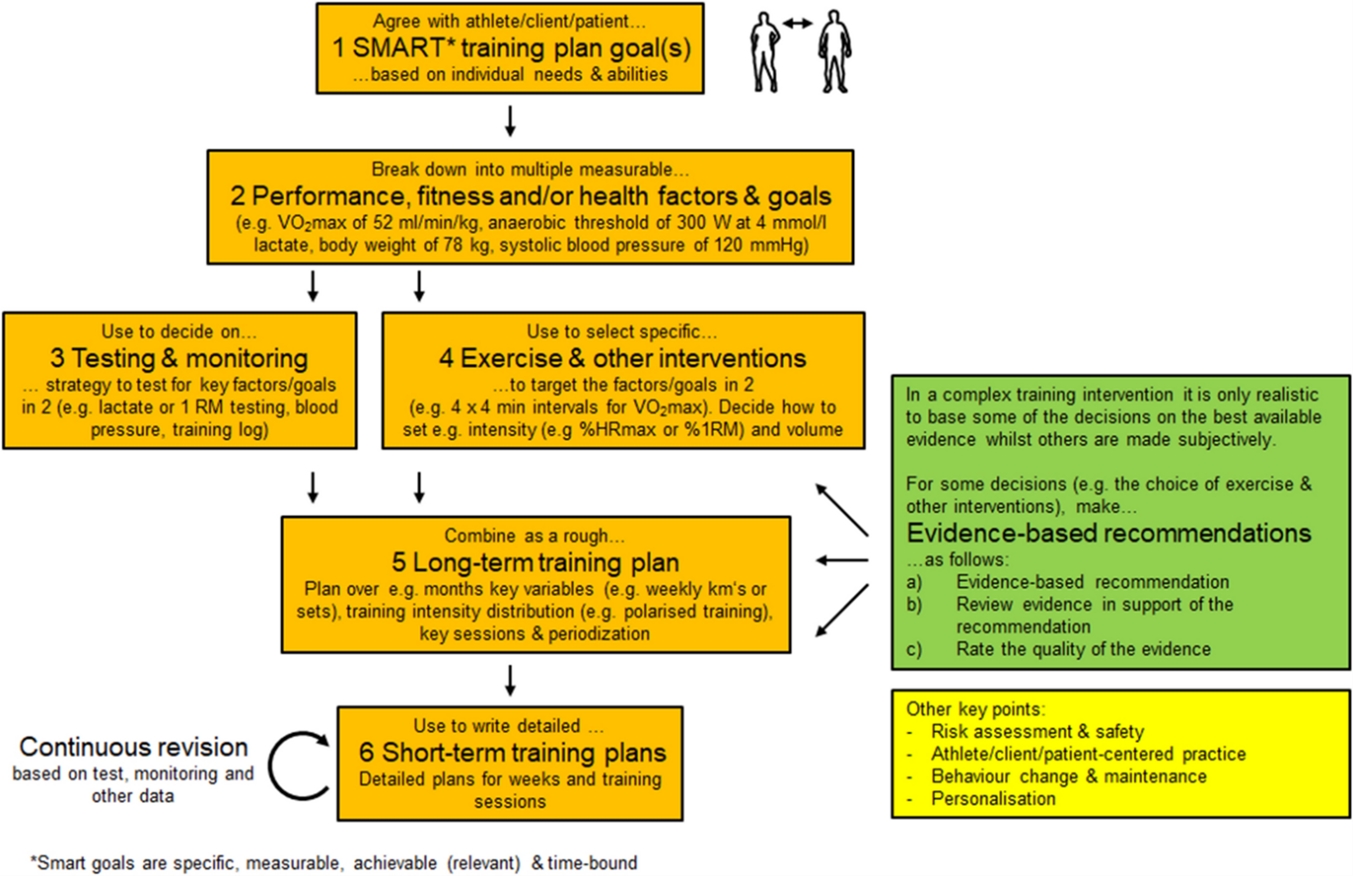
Researchers at the Technical University of Munich in Germany and Lehman College in the USA describe a six-step individualized, evidence-informed exercise training prescription approach(2). The researchers consider the difficulties present in interpreting, adjusting, and applying scientific evidence in practice.- Rehabilitation goals
Practitioners assist athletes in identifying individualized SMART rehabilitation goals. It is critical to understand the athlete’s needs and abilities when developing a rehabilitation plan. Furthermore, competitive level, rehabilitation timelines, and athlete expectations are vital in determining a realistic plan.
- Specify measurable performance, fitness, and health goals.
Understanding the specific athletic sports demands will allow practitioners to develop appropriate performance goals. Performance and general health goals relate to athletic competence and level of participation. The use of universally accepted or evidence-based performance norms (such as the lower limb hop battery, t-sprint, vertical jump test, and the Bronco test) will assist practitioners in developing specific goals.
- Testing and monitoring
The performance goals and indicators specified in steps one and two will determine the testing and monitoring strategy. For example, self-report pain questionnaires, range of motion, and perception of effort during exercise may guide early rehabilitation prescription. As the athlete progresses, practitioners can introduce objective measures such as strength and movement quality tests.
- Therapies and Interventions
Using the performance goals and indicators in steps one and two will determine the therapies and interventions selected by the practitioners. Early rehabilitation aims to reduce pain and inflammation while restoring function. The short-term goals, clinical experience, and athlete preferences will determine treatment selection. General health management is vital during the initial recovery phases through contralateral training effects and general strength and conditioning exercise (e.g., arm cycling for clients with lower limb injuries). As an athlete progresses, training shifts to developing maximal tissue capacity, reactive strength, and coordination.
- Long-term rehabilitation plan
A long-term plan should provide an overview of the complete rehabilitation process. The program should specify the therapeutic options, training modalities, and exercise prescription principles vital for each rehabilitation phase. However, while the long-term plan provides the athlete and practitioners with an overview of the complete process, it may change depending on the client’s response throughout rehabilitation.
- Specific short-term rehabilitation plans
Short-term plans should detail what happens on a weekly or per session basis. Practitioners should monitor and adjust the short-term plans based on the testing and monitoring strategy in step three. Practitioners may need to manipulate the rehabilitation program if the athlete is responding adversely to the short-term plan.
Figure 3: Schematic detailing how to develop an evidence-informed training plan(2).
SUMMARY
There are multiple variables that practitioners need to consider when designing an injury rehabilitation plan. It is challenging and time-consuming to utilize all the available evidence to make decisions. Instead, rehabilitation professionals should aim to be evidence-informed, rely on their clinical experience, and understand the athlete’s preferences. The testing and monitoring strategy must be clear, objective, reliable, and appropriately implemented to ensure a positive rehabilitation outcome. This responsive approach is the best bet to provide a positive outcome.REFERENCES
- (1996) 312:71–2.
- Sports Medicine (2021) 51:1805–1813

Jason Tee

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up
Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.