You are viewing 1 of your 1 free articles
Demands of Sport: Part II – Force your way to the top
Assessing the countermovement jump provides clinicians insight into the tissue capacity during rehabilitation and may guide decision-making. In part one, Helen Bayne discussed force plates, their use, and applicability within the clinical rehabilitation context. In part two, Helen uncovers how to assess asymmetry and interpret the testing results to improve return to sport decision-making. 
Minnesota Twins center fielder Byron Buxton jumps up and attempts to catch a home run from Boston Red Sox right fielder Hunter Renfroe (not pictured) in the fifth inning at Target Field. Mandatory Credit: Jesse Johnson-USA TODAY Sports
The countermovement jump (CMJ) provides clinicians with an easy-to-use, practical, and sport-relevant tool to assess tissue capacity and performance throughout rehabilitation. Return to sport (RTS) assessments typically compare the involved side to the uninvolved side. Practitioners score popular functional tests according to the number of repetitions to failure (e.g., single-leg squat test), the number of repetitions within a specific time limit (e.g., single-leg side-hop test), or the maximum jump height or distance (e.g., horizontal single-leg hop test)(1,2). While these outcome measures provide valuable information about the overall capacity of the patient, clinicians may be unable to detect other neuromuscular changes present after injury. For example, the horizontal single-leg hop test does not indicate symmetrical lower limb kinematics or kinetics in patients who have undergone anterior cruciate ligament (ACL) reconstruction. Patients tend to offload the knee joint to favor the hip and ankle(3).
Most clinics do not have the resources to easily assess joint kinematics and kinetics and report on those variables in a reasonable time frame. However, the increasing viability of force plates that measure vertical ground reaction force presents practitioners with a tool to provide objective data in real-time. Data obtained from force plates can inform the practitioner about mechanical determinants and movement strategies during vertical jumping and landing tasks. There is growing evidence of interlimb asymmetry in previously injured athletes, with the dominant focus on the performance of the CMJ during rehabilitation after ACL reconstruction(4,5,6).
Read More





Asymmetry
As described in part I, when athletes perform the CMJ on force plates, practitioners use the force-time data to identify functional phases within the jump – namely, the unweighting, braking, and propulsion phases. If a dual force plate system is available, practitioners can interpret data for both limbs. In addition, practitioners can calculate multiple metrics from the force-time data, but selecting context-appropriate outcomes remains a challenge(7). However, several metrics demonstrate good reliability, and there is evidence of their importance following severe lower limb injury(4,5,6,8).
Comparison between limbs during a bilateral CMJ reveals decrements in peak vertical force, force at zero velocity (the lowest point of the CMJ), braking impulse, and the propulsion impulse following injury. These decrements are most significant early on in the rehabilitation period (e.g., <6 months post-ACL reconstruction) but can persist for more than two years, even after athletes return to full training and competition(5,6).
One leg or two?
Force production during a bilateral test is not necessarily an indication of each limb’s strength or maximum capacity. Therefore, when practitioners interpret the results from bilateral tests, they should not assume that lower force and impulse values reflect lower strength. Athletes are required to perform unilateral tests to assess each limb. In addition, unilateral CMJs can reveal different force production patterns between the limbs, which may not be evident in bilateral jumps (see figure 1).
Figure 1: The comparison between the bilateral and unilateral CMJ
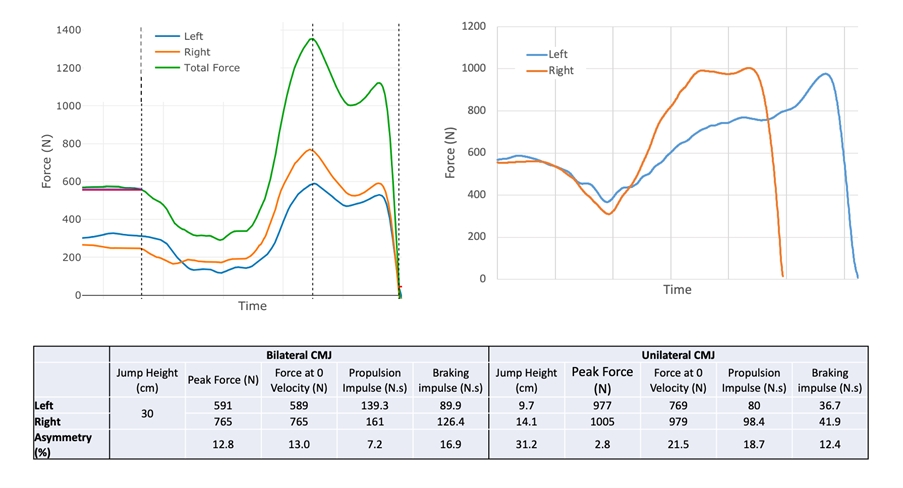
There is a similar pattern of force production on both limbs during the bilateral CMJ with decreased force and impulse produced by the left leg. However, during the unilateral CMJ, marked differences in jump strategy are evident, with a longer duration from initiation to take-off and peak force occurring very late in the propulsion phase on the left leg. In addition, although peak force is similar between the limbs, all other measures are significantly lower on the left leg, and these asymmetries are more significant than those recorded during the bilateral test. This example highlights the value of unilateral testing and the importance of examining multiple metrics and the force-time curve shape.
Unilateral CMJs have not been included in post-injury research studies as often as the bilateral version of the test. However, researchers at the University of Wuppertal in Germany included bilateral and unilateral CMJs in assessing ACL-reconstructed patients between 21 – 42 months after surgery(4). The researchers separated the participants into two groups based on their subjective knee function (International Knee Documentation Committee 2000 Subjective Knee Form). The study results demonstrate that the force at zero velocity was lower on the involved limb than the uninvolved limb in the low knee function group. However, there were no between-limb differences in the high knee function group.
Practitioners require different equations to calculate asymmetry as a percentage depending on whether a unilateral or bilateral test is used(9). Asymmetry must be expressed relative to the total force during bilateral tests, whereas in unilateral tests, this is not the case (see table 1).
Table 1: The equations to calculate lower limb asymmetry as a percentage
| Test Type | Asymmetry Calculation |
|---|---|
| Bilateral | (Right — Left) / (Right + Left) x 100 |
| Unilateral | (Stronger — Weaker) / Stronger x 100 |
Note: Clinicians can replace Left/Right with Dominant/Non-dominant or Involved/Uninvolved. Practitioners interpret the direction of the asymmetry accordingly as positive or negative.
Is symmetry the goal?
One needs to be careful when setting symmetry as the objective. Due to detraining, global strength or performance capacity changes may also have occurred after injury. Alternatively, low strength levels before the injury may have been contributing factor. So, the uninvolved limb may not be a high enough benchmark for establishing complete recovery, addressing pre-injury musculoskeletal issues, or reducing reinjury risk. For example, although more significant between-limb asymmetries exist following injury in athletes with low knee function, the force at zero velocity and braking impulse is greater when athletes report high knee function(4).
Therefore, practitioners should benchmark against previously uninjured or a comparable high-performing cohort in conjunction with asymmetry assessment. In addition, having a pre-injury measurement of the patient will enhance their RTS assessment analysis. Although this may not be available in typical clinical practice, it is achievable in sports performance systems where the tools are available for routine monitoring.
Recommendations
The assessment of vertical jumps using force plates may be a valuable tool for practitioners to monitor athletes after injury. Bilateral and unilateral versions of the CMJ provide complementary information about the athlete’s capacity and loading preference. In addition, multiple metrics derived from the force-time data enable the measurement of the test outcome (jump height) and the mechanism and strategy used by the athlete. Ideally, practitioners should routinely assess athletes while healthy to provide a reference point for post-injury assessment and utilize asymmetry measures in conjunction with performance benchmarks to enhance the RTS decision-making.
References
- Ann Rheum Dis 2004 Apr;63(4):402-7
- Knee Surg Sports Traumatol Arthrosc. 2006 Aug;14(8):778-88
- Br J Sports Med. 2020 Feb;54(3):139-153
- Orthop J Sports Med. 2017 Jun 20;5(6):2325967117710912
- Scand J Med Sci Sports. 2015 Jun;25(3):e301-9
- Am J Sports Med. 2020 May;48(6):1365-1373.
- Strength and Conditioning J. 2021.
- Translational Sports Med. 2019;2(5):256-262
- Strength and Conditioning J. 2018;40(4):1-6.

Latest Issue

Subscribe Today
Further reading
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up




Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.