Principles of tendon healing apply to the Achilles tendon
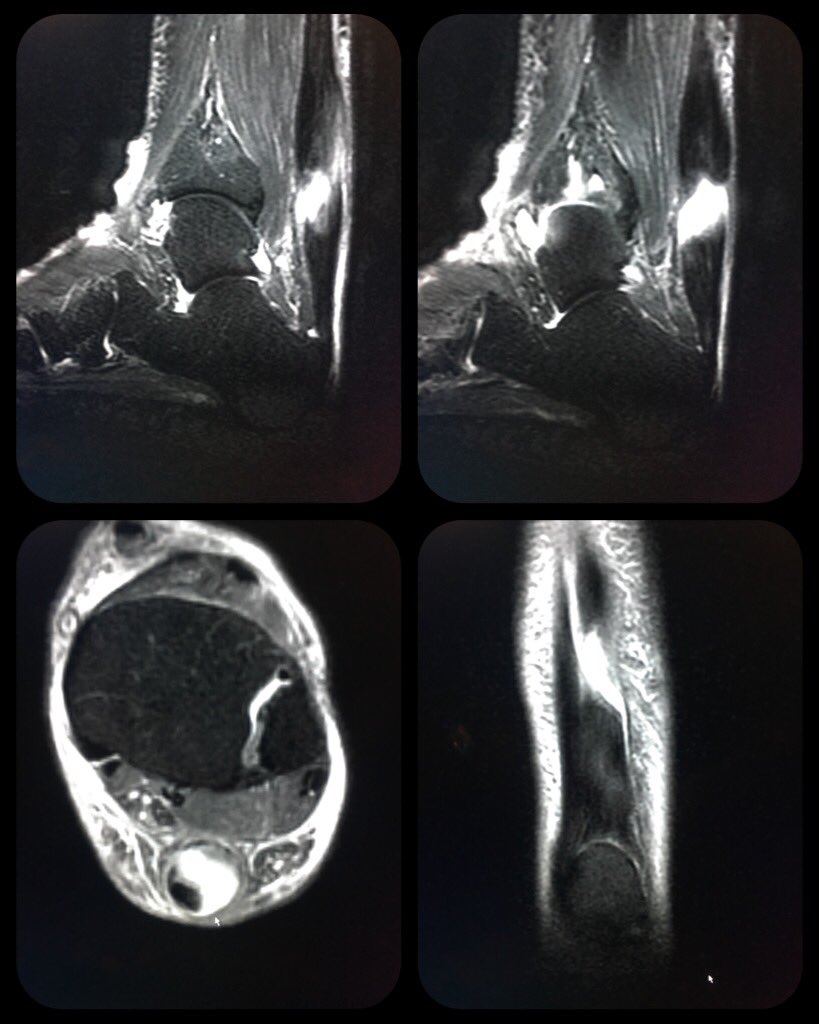
Achilles tendinopathy and tear. Photo Credit William Morrison, MD, @morrisonMSK
The principles of tendon injury and healing apply to any injured tendon, even the Achilles. The largest tendon in the body, the Achilles is the connection for both the soleus and gastrocnemius muscle to the calcaneus. It functions in nearly every activity, including walking, running, jumping, and quick starts and stops. Dutch researchers cite the incidence of mid-portion tendinopathy at 2.35 per 1000 patients registered in a general practitioner practice, with 35% of those cases associated with sports related activities (1). Interestingly, in a study of 102 Achilles tendons in asymptomatic healthy young subjects (mean age about 27 years old), 16% showed abnormal findings on ultrasound. In yet another example of why therapists should treat the patient and not the test, the clinical presentation of tendon pain does not always correspond with imaging results.
Achilles tendinopathy often occurs in the middle of the tendon, an area known as the watershed zone because of the lack of vascularisation in this region. The decreased blood supply makes the tendon here particularly vulnerable to overload injury. Rehabilitation of Achilles tendon injuries, as put forth by Lachlan Wilmot here, is a four-phase process (see table 1). As discussed prior, this approach should take around 12 weeks to complete. The entire process centers around load management. The acute stage focuses on activating the tendon in a way that doesn't stretch it, meaning primarily isometrics. Pain 24 hours after activity dictates how well the tendon tolerated a load, and whether the next activation should be a bit more, a bit less, or the same.
Explaining the mechanics of load management to athletes helps with the perception of activity and understanding of healing. Rather than feel that they've gone back to 'baby' exercises, understanding the different types of tendon loading through different contractions, as discussed by Wilmot here may increase exercise tolerance and acceptance of the rehab process. Tendons can be loaded quite heavily if done using an appropriate method at a suitable time during rehabilitation.
| Table 1: 4-phase progression of Achilles tendon loading | ||||||
|---|---|---|---|---|---|---|
| Phase | Focus | Characteristics | Time Frame | Key Strength Modality | Frequency | Prescription Example |
| - Phase 1 | Acute/Protective | Pain/Stiffness upon wakening Pain on palpation Pain during activity Difficulty performing 10 calf raises | 0-2 Weeks | Isometrics | Daily | Single leg Isometric Hold (heel off step) — Body weight x 20-40 sec x 3 sets Progress to loaded holds |
| - Phase 2 | Load introduction | Pain/Stiffness upon wakening Pain on palpation Reduced pain during activity Pain below a 4/10 when perfoming 10 calf raises | 2-5 Weeks | Isolated ResilienceControlled Eccentrics | Daily to every second day (the heavier the load, the longer recovery time between sessions) | Single Leg Calf Raises (heel off step) x (build up to 20 reps) x 3 sets Eccentric Heel Lowers (heel off step) — 2 legs up, 1 leg down x 10 reps x 3 sets Progress to loaded eccentrics and loaded calf raises |
| - Phase 3 | Strength Accumilation | Pain free upon wakening Reduced pain on palpation Minimal/zero pain with activity Can perform 10 loaded calf raises | 4-10 Weeks | Strength ResilienceReactive Stiffness | Every 2-3 days | Slow Prowler Push x 20 steps x sets BB Step Up — Double Box x 6 reps x sets Mini Tramp Jog x 40 sec ON: 20 sec OFF x 5 sets Knee Drive Hold on BOSU x 20 sec hold x 4 sets |
| - Phase 4 | Elastic Tolerance | Pain free upon wakening Reduced pain on palpation Pain free with activity Jump rope pain free | 10+ Weeks | Reactive StiffnessBallistic Stiffness | Every 2-3 days | Linear hop and stick; 6 reps x 4 sets Lateral hop and stick; 6 reps x 4 setsLinear hurdle and hop; 6 reps x 3 sets Lateral hurdle and hop; 6 reps x 3 sets |
While progressing exercise to rehabilitate the tendon, its important to remember the entire kinetic chain. Tracy Ward explores the importance of core stabilisation in foot biomechanics here and demonstrates many exercises that can be done without adding additional strain on the Achilles tendon. Keeping the rest of the musculoskeletal system, as well as the cardiovascular system, fit while recovering from injury is of primary importance to competitive athletes.
The reason most athletes struggle with tendon healing is the desire to return to play before the tendon is ready. As discussed here, its tempting for them to mask the pain of tendinopathy with the use of NSAIDs in order to return to play faster. Other strategies they may attempt in order to return to sport include platelet therapy. As Andy Hamilton discusses here, the evidence doesn't support the use of platelet rich plasma (PRP) as a therapeutic modality for tendon healing. For now, the tincture of time, combined with progressive load management, is the best medicine.
References:
- BJSM. 2011 Oct;45:1026-28
- Foot Ankle Int. 2018 May 1 [Epub ahead of print]
You need to be logged in to continue reading.
Please register for limited access or take a 30-day risk-free trial of Sports Injury Bulletin to experience the full benefits of a subscription. TAKE A RISK-FREE TRIAL
TAKE A RISK-FREE TRIAL

Alicia Filley

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up
Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.