You are viewing 1 of your 1 free articles
Rate of force development and return to sport following ACLR

2012 South West England's Holly Molesworth in action during the rugby sevens at the Sainsburys 2012 School Games a multi-sport event for 1,600 young people. Credit: Action Images / Paul Childs Livepic
Two-thirds of athletes who undergo ACLR do not return to preinjury sport levels, and three percent to 24% of those that do return end up suffering re-injury or a contralateral anterior cruciate ligament (ACL) tear(1). These statistics are concerning and raise questions regarding the stringency of current return to sport standards.
Quadriceps index testing remains a hallmark measurement of ACLR recovery. This assessment of maximum voluntary isometric contraction (MVIC) via electromechanical dynamometry serves as the gold standard for return to sport decision making. Clinically, handheld dynamometry or one-repetition maximum (1RM) testing of single knee extension or leg press are more readily available options(2). The hop test is the commonly used assessment for lower extremity functional performance. Historically, clinicians strove for a limb symmetry of 90%, but sports scientists now recommend 95% or more before returning athletes to play. However, limb symmetry indexes may overestimate knee function following ACLR and possibly increase ACL injury risk(3).
Why do so many athletes pass these return-to-play tests yet possess a high likelihood of re-injury? Is there another performance variable that physios should address? While the answer is unknown, rate of force development (RFD) deserves serious consideration as the potential missing piece of the puzzle.
Rate of force development
An athlete’s ability to generate force is a critical component of performance. The capacity to produce that force quickly, or RFD, further mimics the demands imposed by sport, especially for athletes who experience limited ground contact during movement. Measured by the maximum steepness of the force-time curve, RFD is divided into an early phase (0-50 milliseconds) and a late phase (>100 milliseconds)(4). The early phase of RFD is related to rapid efferent neuromotor function, whereas the late phase is a function of maximal strength and fiber type composition(4). Both phases are essential for optimal performance; however, the early phase is integral in protecting the ACL.The time required to achieve maximal contraction strength during many sporting activities is <200 milliseconds(1), yet maximum force may take anywhere from 250-800 milliseconds to develop due to electromechanical delay(5). Improving the neural drive in the first 100 milliseconds of muscle activation increases the RFD(4). This timing is significant as most ACL injuries occur within 17-50 milliseconds after ground contact(4). Therefore, adequate muscle activity must occur within a 30-70 millisecond window from the onset of joint loading to effectively protect the ACL(1). Failure to do so may expose the ACL to excessive forces and contribute to non-contact injury(1). Thus, RFD could be a good predictor of the neuromuscular system’s capability to protect the ACL.
Despite the return of the MVIC to pre-injury levels around six months following ACLR, deficits in RFD remain(1). Restoration of pre-injury RFD levels may take up to 12 months, even with 20 weeks of specific training included during that timeframe(1). This time lag highlights the need to look beyond the benchmark achievement of equalized lower extremity strength and continue sport-specific power training before returning an athlete to sport.
Training strategies
One of an ACLR rehabilitation program’s goals is to maximize lower extremity strength, an essential component in developing RFD. While increasing strength through heavy resistance increases RFD, the gains are not appreciable on their own(6). Beyond resistance training, RFD training needs to emphasize explosive movements that attempt to activate the musculature as fast as possible to invoke rapid motor activation(1). Plyometric and ballistic training facilitate quick motor activation through high-force-low-velocity and high-force-high-velocity exercises to maximize power (see figure 1) (1).Figure 1: Comparison of force as a function of time(7)
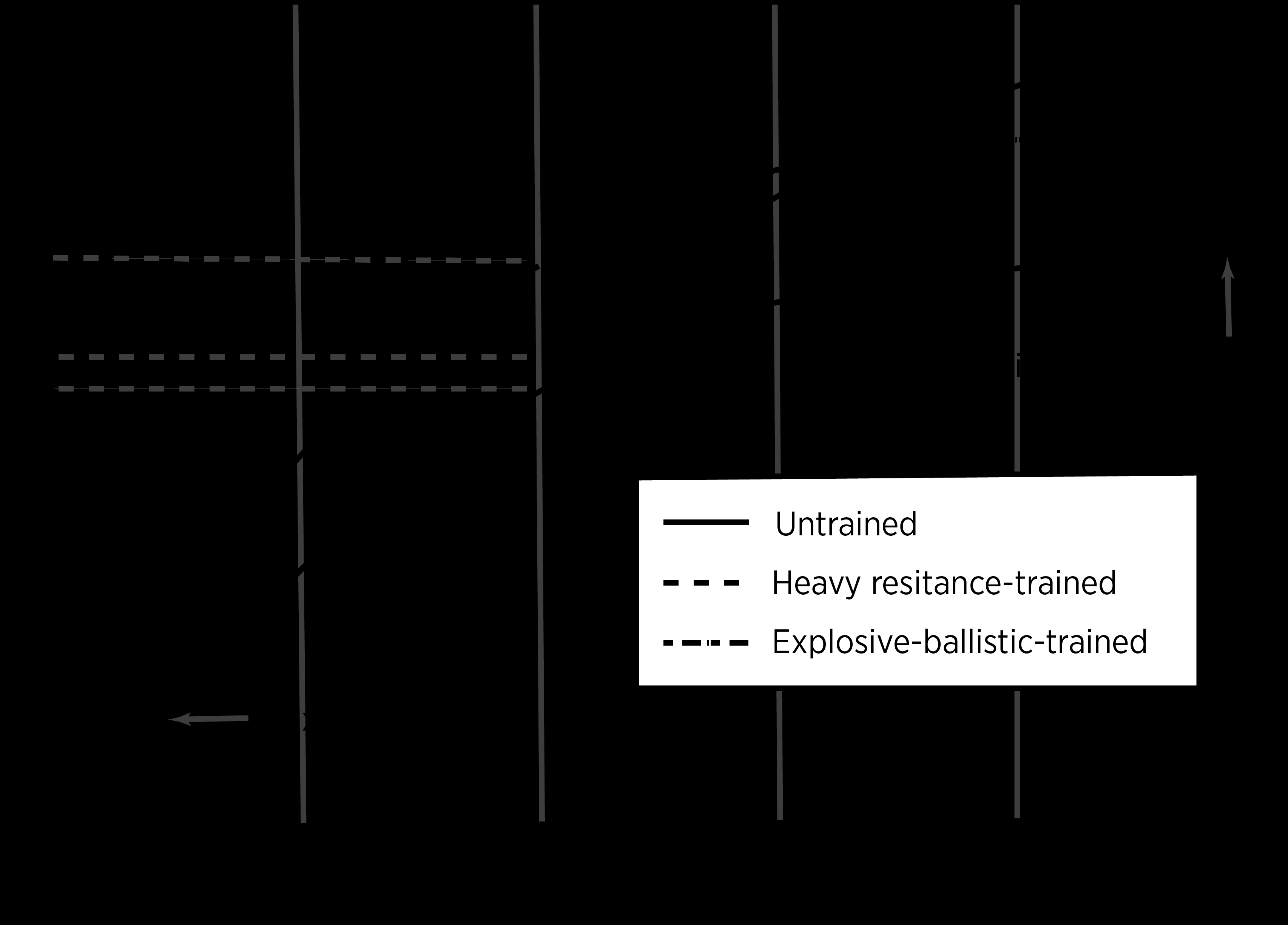
This comparison indicates maximum strength, RFD, and force for untrained, heavy-resistance trained, and explosive-ballistic trained subjects. Adapted from Essentials of Strength Training and Conditioning. Champaign, IL: Human Kinetics; 2016.
Mechanically, plyometric and ballistic training utilize the stretch‐shortening cycle to generate power by using a lengthening, eccentric movement quickly followed by a shortening, concentric movement (see figure 2)(8). Plyometric exercises increase performance by increasing the set speed in which the muscles act, facilitating enhanced automatic neuromuscular coordination(8). Improving automaticity is critical for controlling explosive muscle actions. Such preprogrammed movements leave little to no opportunity for correction during execution(1).
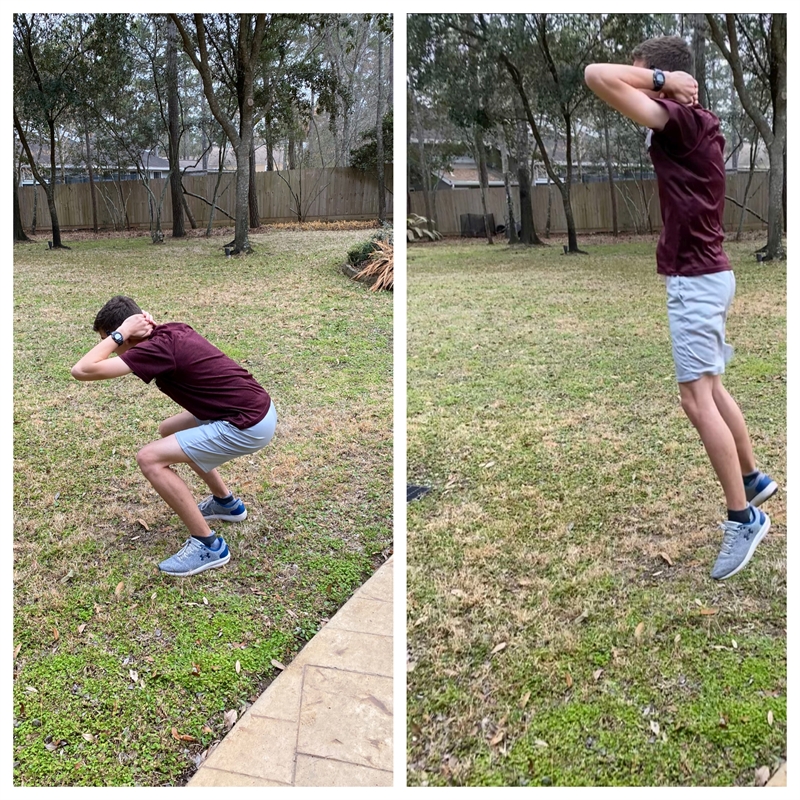
Figure 2. The stretch-shortening cycle applied to a squat jump.

A) Eccentric B) Amortization C) Concentric
A) The eccentric phase preloads the agonist muscle groups, stores elastic energy, and stimulates muscle spindles. B) The amortization or transition phase involves Type Ia afferent nerve synapses with alpha motor neurons which transmit signals to the agonist muscle groups. C) The concentric phase releases stored elastic energy and the alpha motor neurons stimulate the agonist muscle groups(7).
Following ACLR, athletes must meet specific criteria before initiating a plyometric training program to assess readiness and reduce injury risk (see table 1). They should exhibit full, pain-free lower extremity range of motion without swelling. A foundation of strength, balance, and neuromuscular control is necessary to ensure adequate coordination and motor control before exposure to the high demands of plyometric exercises(8).
| Pain | No pain in lower extremities |
| Range of Motion | Full ROM of all joints |
| Swelling | None |
| Balance | 30 seconds eyes open and eyes closed |
| Muscle Strength | 20% bilateral comparison |
| Muscle Endurance 20% bilateral comparison | Neuromuscular Control Good qualitative movement patterns, no compensations |
| Single-Leg Half Squat | Pain-free, good qualitative movement patterns |
| Free Weight Squat (1.5-2.5 body mass) | Pain-free, good qualitative movement patterns |
| Squat (60% body mass, 5 times in 5 seconds) | Pain-free, good qualitative movement patterns |
| Low-Level Plyometric Drills | Pain-free, good qualitative movement patterns |
Despite former training status, treat all athletes following ACLR as beginners when initiating plyometrics (see table 2). Progress drill volume from low to high, decreasing the volume as exercise intensity increases (see table 3). To focus on increasing RFD, instruct athletes to perform each contraction as fast as possible to achieve high peak forces(9). Provide verbal cues to contract “fast and hard” with emphasis on the explosiveness of the contraction(9).
| Plyometric Experience | Volume (contacts per session) |
|---|---|
| Beginner | 80-100 |
| Intermediate | 100-120 |
| Advanced | 120-140 |
Adapted from Essentials of Strength Training and Conditioning. Champaign, IL: Human Kinetics; 2016.
| Exercise Intensity | Volume (contacts per session) |
|---|---|
| Low | 400 |
| Moderate | 350 |
| High | 300 |
| Very High | 200 |
Adapted from Int J Sports Phys Ther. 2015;10(6):760-786.
Youth considerations
Children on the playground naturally perform plyometric activities such as skipping, hopping, and jumping during free play(10). Yet, plyometric training may place undue stress on prepubescent athlete’s immature skeletons, specifically open epiphyseal plates. Therefore, avoid depth jumps and high-intensity plyometrics in these athletes to prevent premature closing, fracture, or leg length discrepancy (see figure 3)(7). Otherwise, adolescent plyometric training is safe and effective in enhancing muscular power, neuromuscular control, bone strength adaptations, and performance when provided with appropriate programming and proper supervision(7).As previously mentioned, athletes of all ages need a strong base before beginning a plyometric training program. For adolescents, both chronological age and training age are important considerations in determining readiness. Establish foundational strength then progress to low-volume (80-100 contacts per session) low-intensity drills as tolerated. Exercises should be sport-specific and progress from simple to complex. Pay special attention to technique to minimize injury risk through faulty mechanics. Once proper technique is learned, emphasized fast, explosive performance to develop RFD.
Figure 3: Plyometrics for various age groups(7)
(A) Squat jumps

(B) Squat box jumps

(C) Depth jumps
Squat jumps (A) and squat box jumps (B) are examples of low and moderate intensity plyometric exercises safe for adolescents. Avoid high intensity plyometrics, such as depth jumps (C), in the prepubescent athlete(7).
Summing it up
Deficits in lower extremity RFD occur following ACLR(1). Many athletes return to sport with continued RFD deficits which may contribute toward re-injury. Improve RFD through plyometric drill training with an emphasis on fast, explosive muscular contraction. Modify plyometric training for prepubescent athletes using low to moderate intensity drills at low frequency (one to two times per week) while avoiding high-intensity drills and depth jumps. Physios may lack specialized equipment necessary for measuring RFD (i.e., isokinetic electrodynamometer, isometric testing systems, force plates, strain gauges, specialized software). Nevertheless, little to no equipment is necessary to train RFD and doing so may better prepare athletes for return to play after ACLR.References
- J Orthop Sports Phys Ther. 2012;42(9):772-780.
- J Orthop Sports Phys Ther.2017;47(2):97-107.
- J Orthop Sports Phys Ther. 2017;47(5):334-338.
- J. Sports Med. 2020;48(13): 3214–3223.
- UKSCA 2009;14: 20-32.
- J Appl Physiol 2002;93:1318-1326.
- Essentials of Strength Training and Conditioning. Champaign, IL: Human Kinetics; 2016.
- Int J Sports Phys Ther. 2015;10(6):760-786.
- Eur J Appl Physiol. 2016;116(6):1091-1116.
- Strength Condit J. 2000;22(3):45-46.
Jessica Montgomery

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up




Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.